Facultative etiology of Twin–Twin Transfusion Syndrome
Monochorionic twins may be viewed hemodynamically as two pumps connected in parallel via placental vascular anastomoses. The hemodynamic equilibrium is maintained as long as both fetuses pump the same amount of blood in opposite directions.
Selective pump failure may occur in one of the twins from cardiac dysfunction secondary congenital heart disease, myocarditis or obstruction at the level of the umbilical cord. The affected fetus may not be able to tolerate the additional amount of blood coming from the other twin. As a result, the affected fetus becomes the recipient and the other twin the donor.
The sonographic characteristics of the syndrome in this twin pair may show two important features: 1. The recipient twin may be affected out of proportion to the degree of involvement of the donor twin. For example, the recipient twin may show hydrops, while the donor twin may still show a visible bladder (atypical stage IV disease; see Chapter 7).
2. Further failure of the recipient twin may actually show improvement of the disease, as increased impedance to the flow of blood from the donor to the recipient twin may hinder further blood loss from the donor.
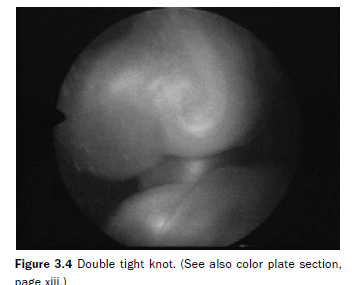
Indirect evidence in support of the facultative etiology comes from a selected group of cases in which the diagnosis of congenital heart disease is made in one of the fetuses. Almost invariably, the affected twin would be the recipient. Of 615 patients assessed at our institution, congenital heart disease was diagnosed in 6 fetuses (0.9%), mostly pulmonary artery stenosis (Table 3.3). An additional 3 patients had abnormalities of the umbilical cord, which presumably could also hinder blood return to the donor, or impair oxygenation in the recipient from obstruction of the umbilical vein, resulting in congestive heart failure of the recipient. One of the patients with cord abnormalities had a double tight knot (Figure 3.4). The other two patients had an umbilical cord kink. In all but one case, the fetus with either congenital heart disease or umbilical cord obstruction was the recipient.
Facultative etiology could also result from a donor twin with increased placental impedance as a result of decreased placental mass. Initial elevation of the blood pressure in the donor to improve perfusion of the reduced placental mass could result in an excessive amount of blood being forced through the vascular anastomoses to the recipient twin. Excessive blood loss to the recipient would perpetuate the cycle.
Estimation of the net blood volume exchange
Direct assessment of the net blood flow exchange between the donor and the recipient twins has not been possible thus far. Although our endoscopic study for the DR score showed an apparent greater size or number of AV anastomoses from donor to recipient, this approach cannot be used to quantify the actual amount of blood flow exchange.

Blood returning through the umbilical vein represents the sum of blood sent by one fetus to the placenta plus the amount of blood received from its co-twin minus the blood lost to the co-twin.
Assessment of the net blood flow exchange could be addressed in two different ways:
• comparing umbilical venous blood flow before and after complete laser obliteration of the vascular anastomoses
• estimating the blood flow exchange at the level of the anastomoses themselves.
The combined cardiac output of the right and left ventricle is 100–500 ml/min for 20–28 weeks’
gestation.5 Of that, 40–45% is directed into the placenta. There are approximately 12–30 individually perfused cotyledons.1 Thus, the amount of blood flow in the umbilical vein ranges between 40 and 200 ml/min, and the amount of blood flow through each cotyledon approximately 1.3–16.6 ml/min. In addition, there are approximately 50–60 main stem villi present in the placenta. 1 Thus, the blood flow volume through each main stem is approximately 0.3–3 ml/min. These figures serve as a reference to understand the results of sonographic estimates of blood flow exchange between the fetuses.
Assessment of umbilical venous blood flow before and after laser obliteration of all vascular anastomoses
We conducted a study to evaluate total umbilical venous flow (TUVF) before and after SLPCV.6 Forty-one TTTS patients were assessed sonographically before and 24 hours after surgery. The umbilical vein was sampled in a free loop close to the abdominal wall insertion. The diameter of the umbilical vein was measured from ‘inner to inner’ in a section of the vessel perpendicular to the ultrasound beam. Measurement of the time-averaged velocity was done with an angle of insonation as close to 0 degrees as possible. All measurements were made in the absence of fetal movements or breathing. Angle correction for measurements was performed where necessary.
TUVF was calculated as follows:
TUVF (ml/min) = mean venous time-averaged velocity (cm/s) ? mean cross-sectional area (cm2) ? 60 s.
TUVF was significantly higher in the recipient (111.2 ml/min) than in the donor twin (44.8 ml/min) before SLPCV (p < 0.0001). However, TUVF was no different between recipient and donor twin after SLPCV (93.1 ml/min vs 70.7 ml/ min, recipient and donor twin, respectively (p = 0.11). The donor’s TUVF increased after surgery (p < 0.0001), while the recipient’s TUVF decreased (p = 0.041) (Figure 3.5). The median postoperative increase in the donor’s TUVF 25.9 ml/min had a corresponding decrease of TUVF in the recipient twin 18.1 ml/min (p = 0.27). Assuming an average of 4–5 vascular anastomoses in each placenta, the blood flow through each anastomosis would be approximately 4.4 ml/min.
These estimates are in agreement with classic physiology and surgical pathology data, as noted above.
Assessment of net blood flow exchange by ultrasound interrogation of the individual vascular anastomoses via intra-amniotic ultrasound
The net blood flow exchange between the fetuses can also be estimated from the algebraic sum of the individual vascular anastomoses. To do this, insonation of each anastomosis is required. Because transabdominal ultrasound lacks the necessary resolution to identify each and every vascular anastomosis, we conducted a study using direct sonographic assessment of the vessels via intra-amniotic ultrasound.7 Patients with TTTS, an anterior placenta, and without superficial placental vascular anastomoses undergoing laser therapy for TTTS were considered eligible for the study.
After adequate endoscopic documentation of all vascular anastomoses, an 8.5 MHz diagnostic ultrasound catheter (ACUSON AcuNav, Siemens Medical Solutions, Inc., Mountainview, CA) was inserted into the amniotic cavity through a separate 2 mm port. Under endoscopic guidance, the catheter was placed directly beneath each arteriovenous


(AV) anastomosis (from donor to recipient, AVDR, and from recipient to donor, AVRD) (Figure 3.6). Color flow images and pulsed Doppler waveforms of the arterial component of the AV anastomoses were obtained (Figure 3.7). The diameter of the artery was measured from the color flow mapping image. Arterial blood flow volume was calculated offline. Net blood flow exchange was calculated as: Total AVDR flow ?
Total AVRD flow

The protocol was approved by the Institutional Review Board of St. Joseph’s Hospital in Tampa, FL, USA and all patients gave written informed consent.
Three patients agreed to participate in this study. Complete measurements could be obtained in two of them. Table 3.4 shows the individual blood flow values in each of the assessed anastomoses. The net blood flow was 1.6 ml/min and 11.6 ml/min in the two patients measured. However, contrary to expectations, the calculated net blood flow was from recipient to donor in both cases. Although the study was significantly limited by the focal length of the ultrasound transducer, the orders of magnitude were again within those expected.
Ultrasound estimate of the net blood flow exchange using TUVF agreed with the fundamental hypothesis of TTTS, with estimates of the exchange consistent with classic physiology and surgical pathology data. Estimates using intraamniotic ultrasound were limited by technical reasons, perhaps explaining the contradictory results, but were also within the same order of magnitude. Future work in this area will probably be geared to improving the accuracy of blood

flow estimates at the level of the individual anastomoses with better technology.
Thank you for this.
ReplyDelete